One abortionist says:
“I tell my patients, don’t come see me again. You should learn your lesson this time.”
E Dorsey Smith Abortion: Healthcare Perspectives (Norwalk, Connecticut: Appleton – Century Crofts, 1982) 193
Share on FacebookThey said it.

One abortionist says:
“I tell my patients, don’t come see me again. You should learn your lesson this time.”
E Dorsey Smith Abortion: Healthcare Perspectives (Norwalk, Connecticut: Appleton – Century Crofts, 1982) 193
Share on FacebookFrom a woman who spoke about prolife issues in schools:
“… We discussed abortion and euthanasia, and I noticed that many of the 8th graders who labeled themselves “pro-choice” were horrified when they learned the truth about these practices. It made me realize how much the “pro-choice” position is against human reason and how much it relies on tired rhetoric to succeed.”
Erin Campell, of Ann Arbor, Michigan, interning with the Life Legal Defense Foundation in Napa, California
Lifeline, Fall 2002 Quoted in Intecon Abortion: Pros and Cons (Bloomington, IN AuthorHouse, 2004)
The Lifeline article did not reveal what information Campbell gave to the 8th grader’s, but below are some pictures that show the reality of abortion.

Before abortion

After abortion
How many “pro-choicers” know the reality of what is shown above?
Share on FacebookFrom a woman whose unborn baby tested positive for Down syndrome:
“I was looking forward to this child until I got the news that the baby had Down syndrome. Then, the child became an “it”… I was so defective that I couldn’t produce a non-– defective baby. I felt that if people knew, they would be horrified and I would be shunned.”
Angela Lanfranchi, Ian Gentles, Elizabeth Ring – Cassidy Complications: Abortions Impact on Women (Ontario, Canada: The deVeber Institute for Bioethics and Social Research, 2013) 151
Share on FacebookIn one article on performing late term abortions:
“We use urea to be certain that we effect fetal death. It is unsettling to all personnel to deliver these fetuses when they are not stillborn.”
R Wachbroit and D Wasserman “Patient Autonomy and Value Neutrality Nondirective Genetic Counseling” Stanford Law & Policy Review 1995; 6 (2): 103 – 11
Quoted in Angela Lanfranchi, Ian Gentles, Elizabeth Ring – Cassidy Complications: Abortions Impact on Women (Ontario, Canada: The deVeber Institute for Bioethics and Social Research, 2013)
Share on Facebook“It cannot be comfortable for the fetus to have a scalp electrode implanted on his skin, to have blood taken from the scalp or to suffer the skull compression that may occur even with spontaneous delivery. It is hardly surprising that infants delivered by difficult forceps extraction act as if they have a severe headache.”
Valman & Pearson, “What the Fetus Feels,” British Med. Jour., Jan. 26, 1980
Share on Facebook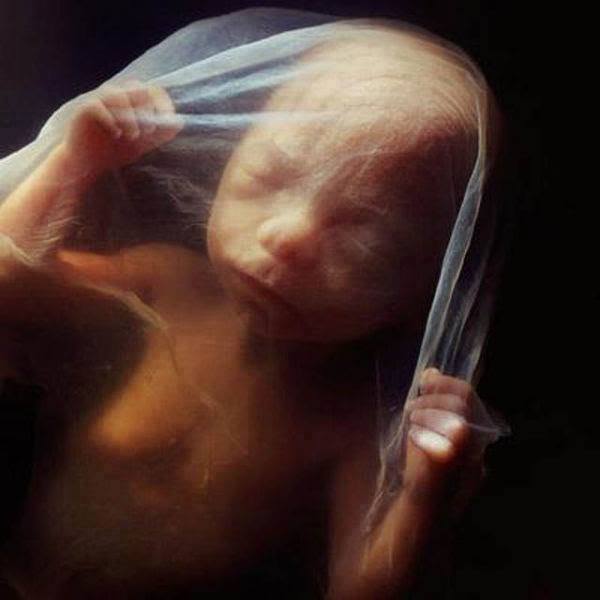
As early as 18 weeks, stress hormones are released by an unborn child injected by a needle, just as they are when adults feel pain. Hormone levels in those babies decrease as pain-relievers are supplied.
Garg, A & Rovnaghi, C. “Fetal Response to Intra-Uterine Needling: Is It Pain? Does It Matter? Pediatric Research. V 51, No 1, 2002.
Share on FacebookPioneer in fetal development M. Liley talks about how the baby in the wombk can experience an uncomfortable or comfortable feeling.
“One of the most uncomfortable ledges that the unborn can encounter is his mother’s backbone. If he happens to be lying so that his own backbone is across hers [when the mother lies on her back], the unborn will wiggle around until he can get away from this highly disagreeable position.”
M. Liley & B. Day, Modern Motherhood (Random House, 1969) 42
Share on FacebookLate term abortionist Warren M. Hern wrote a textbook on how to do abortions. He describes different ways to abort babies:

“Once the tissue is grasped, the forceps is withdrawn gently with a rotating motion to permit easier passage. If any doubt is entertained about the kind of tissue being grasped, the rotation should occur before withdrawal. If uterine wall or viscera is between the forceps blades, it will not rotate easily and the patient will experience discomfort. The tissue can be released and damage minimized. The forceps should be applied with extreme caution to avoid the latter calamity. The probability of difficulty in removing the 1calvaria [human skull] is greater at 15 weeks than at any other time. Continuing to search or attempt to grasp without success is increasingly dangerous with time, because the uterine wall is more and more likely to become the tissue that is grasped. As the calvaria [human skull] is grasped, a sensation that it is collapsing is almost always accompanied by the extrusion of white 2cerebral material…This calvaria sign [white cerebral material] may not be much in evidence with the 13-week procedure, but it is more likely to appear at 14 weeks.”

… At 16 to 17 weeks, fetal tissue is much more easily identifiable with the forceps and in some ways is easier to grasp and remove than in earlier gestations. The [skull] is about the size of a Ping-Pong ball and usually can be grasped readily with the Bierer. Collapsing it gives a definite sensation… At 18-19 menstrual weeks… fetal parts are significantly larger and more difficult to morcellate (tear into pieces)… [Abortion after] 20-week gestation… can be a significantly more difficult procedure accompanied by unnerving hemorrhage. Forceps use must be sure and relatively rapid. There is frequently not much time for exploring the nuances of different tissue sensations. Grasping and collapsing the [skull is] often difficult. Stripping the [skull] of soft tissue is sometimes the first step in successful delivery of this part, followed by dislocation of parietal bones. In this case, care must be taken in removal because ossification is occurring and the edges are sharp… Regardless of the amount of dilatation, delivery of the [skull] and pelvis is sometimes difficult… The advantage obtained by having a softened cervix could become a disaster if a laceration develops at the level of the internal os as the result of too much force…

The procedure changes significantly at 21 weeks because the fetal tissues become much more cohesive and difficult to dismember. This problem is accentuated by the fact that the fetal pelvis may be as much as 5 cm in width… [The skull] can be collapsed. Other structures, such as the pelvis, present more difficulty.
The calvaria is no longer the principal problem; it can be collapsed. A long curved Mayo scissors may be necessary to decapitate and dismember the fetus. After the bimanual examination, the physician removes the basin from beneath the patient’s perineum and replaces her feet on the pull-out leg support. At this point, I move around the table to face the patient, to inform her that she is no longer pregnant and to reassure her. Many patients are prepared to cry. The aggregate fetal tissue is weighed, then the following fetal parts are measured: foot length, knee-to-heel length, and biparietal diameter. In most cases, the calvaria has been collapsed but is basically intact. It is placed under running water and, as the water fills the cranium, a biparietal measurement is taken by sight with a clear plastic ruler.”
Warren M. Hern. Abortion Practice (Philadelphia: J.B. Lippincott Company, 1990), 150-154
Share on FacebookLate term abortionist Dr. Warren Hern was interviewed for an article in Esquire. He told the following story:
“The patients can be upsetting too. They’re under terrible stress, of course, but sometimes they come in very angry. One had conjoined twins and would have died giving birth, but she exploded when he told her she couldn’t smoke in the office… One even said they should all be killed. Only fourteen, she came with her mother. What brings you here? he asked, I have to have an abortion. Why? I’m not old enough to have a baby. But you told the counselor we should all be killed? Yes, you should all be killed. Why? Because you do abortions. Me too? Yes, you should be killed too. Do you want me killed before or after I do your abortion? Before.
He told her to leave. Her mother was very upset. But he isn’t an abortion-dispensing machine. He’s a physician. He’s a person.”
John H. Richardson “The last abortion doctor” Esquire September 1, 2009
While what the teen said is horrible, one thing to take away is that she was no doubt being forced into the abortion by her mother. She must’ve known that if she said that to the doctor, he would not perform it – perhaps that’s why she said it. One wonders if Dr. Hern would’ve performed the abortion on this teen and sent her home if she had not insulted him. He could’ve done an abortion against her well and sent her home to suffer the emotional consequences if she had not spoken out in an alarming way.

See Dr. Hern’s website to see him advertise to abort babies as old as the one above (and older).
Share on FacebookWhen Ronald Reagan was president, he made a statement that pre-born babies being aborted suffered agonizing pain. Immediately, pro-choice groups attacked his words, claiming that it wasn’t true.
But twenty-six medical authorities, including two past presidents of the American College of Obstetricians and Gynecologists wrote a letter:
“Mr. President, in drawing attention to the capability of the human fetus to feel pain, you stand on firmly established ground…. That the unborn, the prematurely born, and the new-born of the human species is a highly complex, sentient, functioning, individual organism is established scientific fact…. Over the last eighteen years, real time ultrasonography, fetoscopy, study of the fetal EKG [electrocardiogram] and the fetal EEG [electroencephalogram] have demonstrated the remarkable responsiveness of the human fetus to pain, touch, and sound.”
Letter to President Reagan, cited by John Willke in Abortion Questions and Answers (Cincinnati, Ohio: Hayes Publishing Co, 1988), 169.
Share on Facebook